CASE STUDY
Planning a Total Knee Revision
Case presented by Krishna Tripuraneni, MD Orthopaedic Total Joint Replacement Surgeon at New Mexico Orthopaedics in Albuquerque.

Industry
Healthcare
Key solutions
OrthoView
The impact
Quick and easy preoperative planning
Higher accuracy and predictable patient outcomes
Krishna Tripuraneni, MD is a fellowship-trained orthopaedic surgeon at New Mexico Orthopaedics in Albuquerque, NM, specializing in total knee and hip replacement. He uses digital preoperative planning to prepare all of his total joint procedures and has been using OrthoView for six years.
The challenge
Establish a surgical plan for a total knee revision
The patient was an 86-year-old woman who was the primary caregiver for her husband and had previously been an active person in the local community. She was experiencing increasing right knee pain and deformity and was unable to walk without the use of a cane. Even mundane daily activities were considerably more challenging as a result of her right knee pain and swelling.
A physical examination revealed anteroposterior and medial instability with 10-degree hyperextension to 90-degree flexion. Due to gross component loosening on radiographs and functional limitations, a revision knee procedure was planned.

The solution
OrthoView preoperative planning software
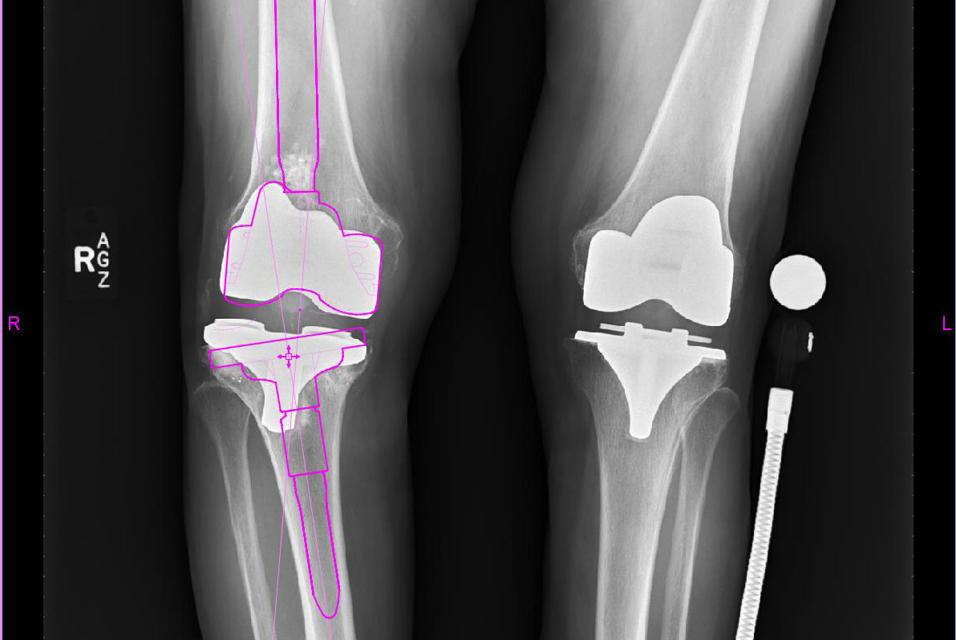
Using the OrthoView preoperative planning solution, the following preoperative considerations were identified and incorporated into the surgical plan:
Components:
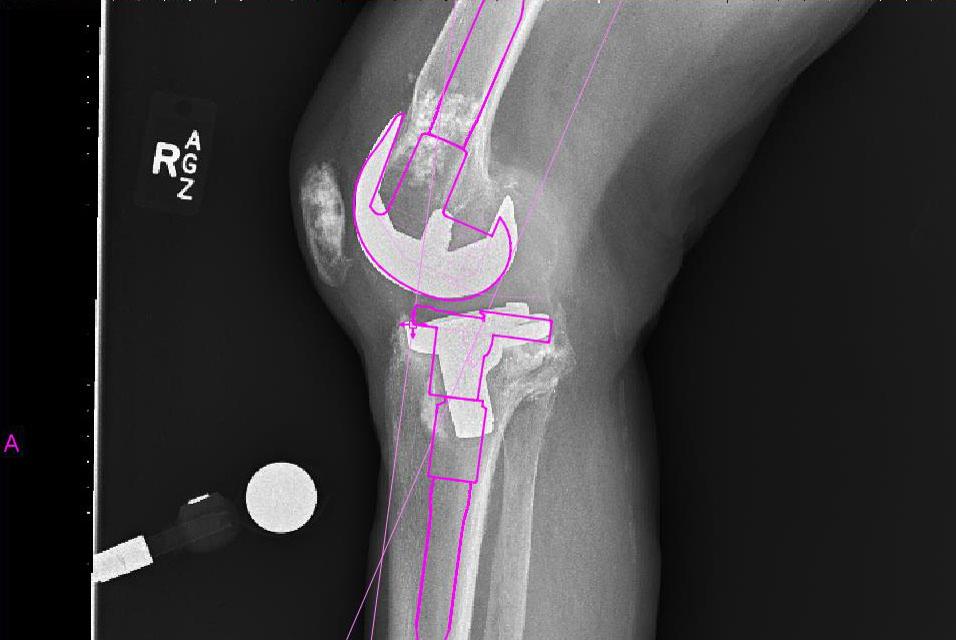
- It was identified that stemmed components were required for both the tibia and the femur.
- We determined that a tibial augment was required as a result of the varus failure of the tibial component and medial tibial bone loss.
- The offset value provided by the software identified that an offset tibial component was required to avoid an abutment of the cortex by the tibial stem.
Joint line:
- We were able to assess how the preoperative plan would affect the joint line and determined that it would maintain it reasonably well.
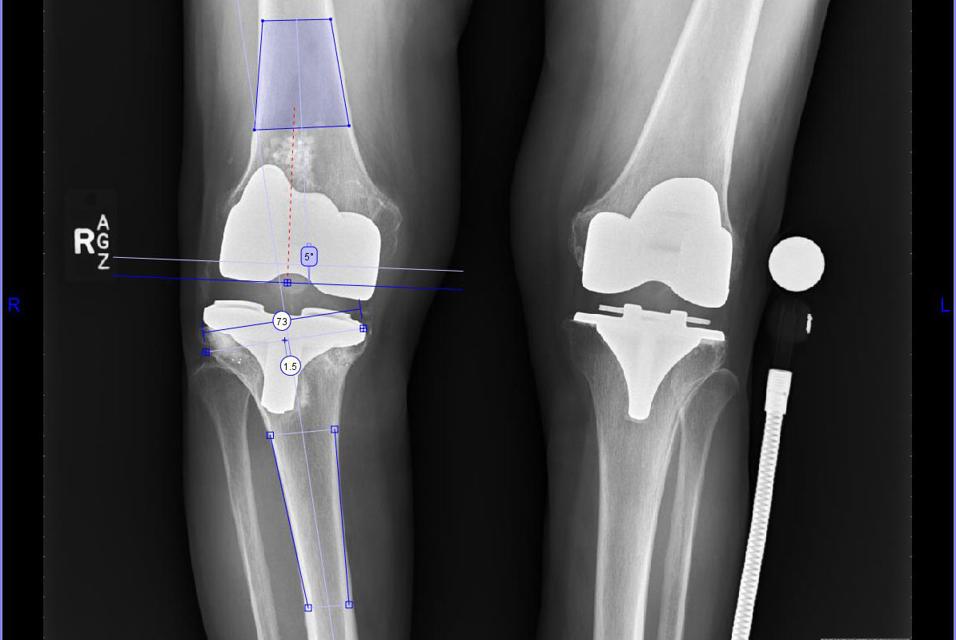
In revision cases, the existing femoral and tibial component positions are ignored, and bony landmarks are used to identify where to place the femoral and tibial preoperative planning tools.
There appeared to be a significant amount of osteolysis in the femur. Metaphyseal cones or allografts were considered for bone stock restoration/substitution, but were eventually not needed.
The preoperative planning software allows the width of the femur and tibia to be assessed for proper component sizing, which is important as size is the primary focus, rather than angles. Intramedullary guides are used to restore the mechanical axis. Also key with revisions is identifying where the articular surfaces of the revision components would lie, in relation to the shaft. Further, it is helpful to preoperatively determine the offset of the tibial component (more than that of the femoral component), as this can help intra-operatively reduce the need for trialing of various tibial stems.
The tibial AP axis indicates that an offset tibial stem will be needed.
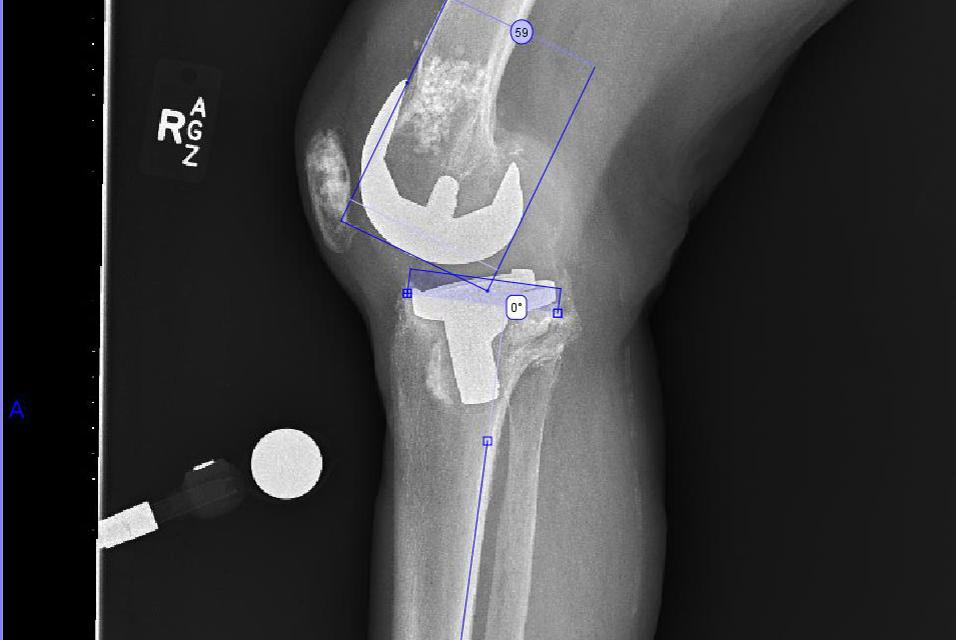
During the templating stage, varying stem sizes are trialed to ensure bony defects will be bypassed by at least two cortical diameters.
Templating on the lateral view permits assessment of the proposed joint line. Augments can readily be added to the distal femur or tibia if the templated polyethylene size is too large, or the joint line is too high or low, based on bony landmarks.
The result
Precision planning for a more predictable patient outcome
Planning this case preoperatively with OrthoView enabled Krishna Tripuraneni to identify several key factors easily: the point at which to stop reaming (to avoid an intraoperative fracture), suitable stem sizes (diameter and length), as well as additional component sizes, the offset requirements for the stem, and the size of stem extension needed to obtain diaphyseal engagement. Digital preoperative planning also made it quick and easy to establish the mechanical alignment of the leg with the use of the SmartKnee Wizard.
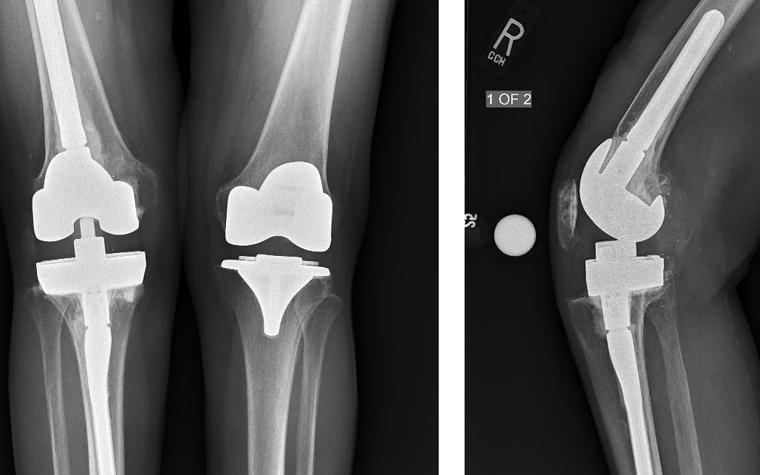
Postoperative critiques:
- As there was intraoperative hyperextension, tibial augments and a 17 mm polyethylene were used to balance the extension space (in addition to distal femoral augments), which caused the joint line to be raised by a few millimeters.
- A hybrid cementation technique was used for this case.
- The postoperative ROM at the one-year follow-up was found to be 0-115 degrees.
Materialise OrthoView is a digital templating solution used by orthopaedic surgeons to quickly and easily create detailed preoperative plans from digital X-ray images. Materialise OrthoView facilitates digital planning and templating for joint arthroplasty and revisions, trauma, limb deformity correction, osteotomies, and spinal assessment and is chosen by hospitals worldwide to complete their target of film-free radiology.
This content is intended for healthcare professionals only.
Featured products and services
Share on: