EXPERT INSIGHT
Artificial Intelligence Cuts Number of Changes to Knee Surgery Planning by 50%

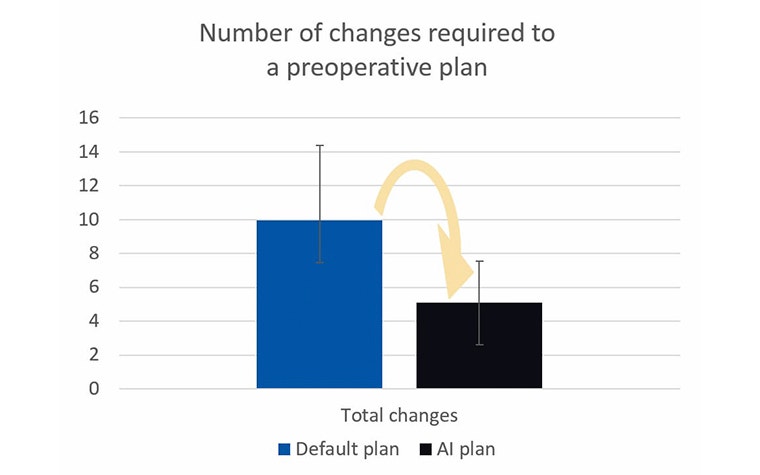
Surgeons would need to make 50% fewer changes to AI-based preoperative plans compared to current ones. This is according to a research project we conducted here at Materialise with Dr. Raf De Vloo, an orthopaedic surgeon at AZ Klina in Belgium, in which we applied AI-based planning to 193 cases. This technology learns an individual doctor’s preferences for surgical approaches and, based on those, provides higher-quality preoperative plans.
We are all becoming more and more accustomed to AI, with voice recognition software on our phones, Netflix recommendations, and email spam filters. But what about AI in healthcare? Though the industry has been slower to adopt the new technology, the first products have hit the market in the last few years, and today almost every company involved in healthcare has AI on its research radar. AI has been used in products that range from finding out if a patient has suffered from a stroke based on a CT scan to discovering irregular heart rhythm and even detecting a disease called retinopathy that affects the eyes of diabetes patients.
During the annual meeting of the American Academy for Orthopedic Surgeons (AAOS) earlier this year, AI was a major topic at almost every preoperative planning discussion. Overall, there was a consensus that this technology has great potential to improve preoperative planning while reducing planning time and decreasing associated costs. At the conference, we were very pleased to present, for the first time, the results of our AI research for total knee arthroplasties (TKA) planning which provides strong evidence and was validated by peers.
AI applied to personalized solutions
AI works by learning how to solve problems without being explicitly programmed how to do so. We saw this could be useful for planning total knee arthroplasties, in which sections of the knee joint are replaced by metal implants to help patients suffering from osteoarthritis.
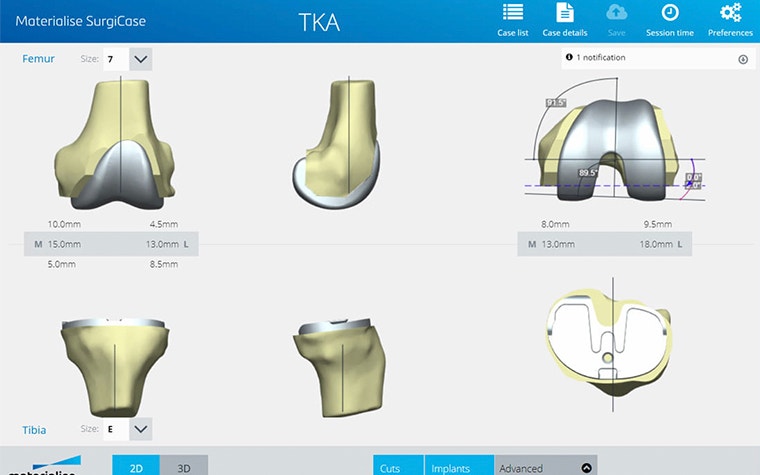
Since 2006, Materialise has provided personalized planning, implants, and guides that help surgeons perform surgeries. We create solutions that are unique to each patient with the help of our planning and communication platform called SurgiCase, in which a doctor can upload a patient’s medical imaging data, plan cases and communicate with a Materialise clinical engineer.

To improve this software solution even further, our research team developed a robust AI algorithm that can automatically detect a surgeon’s preoperative preferences based on their past cases. For this project we collaborated with Dr. De Vloo, a surgeon with more than seven years of experience with personalized solutions developed by Materialise. This research applied our AI-based models to 193 past cases from Dr. De Vloo. The results were remarkable; we were able to reduce the number of corrections the surgeon had to make to his preoperative plans by half. Since then, we have applied this experiment model to multiple other cases from different surgeons, each time with at least a 50% reduction in alterations that the surgeons have to make.
Why use AI for TKAs?
There are many steps involved before having a final surgical plan in place. First, the patient’s knee joint is scanned using computer tomography (CT) or magnetic resonance imaging (MRI) during an examination. Next, these scans are securely transferred to Materialise, where they are used to create a virtual 3D model of the patient’s joint. Materialise then proposes a personalized plan that specifies how the surgeon could place the metal implant components. The preoperative plan is sent to the surgeon for review, and if necessary, they can modify it and send it back to Materialise. Once the surgeon gives their approval, personalized guides are 3D printed. These guides allow the surgeon to place the implant components as planned based on the patient’s anatomy prior to surgery.
The preoperative planning process is quite complex, and due to different schools of thought, surgeons have a variety of approaches for how to place the two metal implant components. This is because the surgeon has 12 degrees of freedom for translation and rotation of the implant components, and there are many different strategies to determine the degrees of freedom.
The majority of surgeons will need to make manual changes in order to adapt the preoperative plan according to their preference. This led us to look into AI to see if this could help us create preoperative plans which are custom to the patient and surgeon. In that way, we can propose personalized solutions that take into account the typical surgical strategy of the surgeon performing the procedure. Doing this will enhance the efficiency of creating personalized solutions, and surgeons would not have to spend a considerable amount of time altering preoperative plans to their surgical preferences.
What’s next?
In the future, we will be working to extend the abilities of AI-based planning and validate this application in a clinical setting. TKA was the first research application for our AI-based planning; however, the methodology is independent of the end application. The goal of our further research is to be able to apply it to preoperative planning for other surgical procedures. Keep tuned for our next AI-based planning announcements.
L-100464-01
Partageons :
Vous aimerez peut-être aussi
Ne ratez jamais une histoire comme celle-ci. Recevez-les dans votre boîte de réception une fois par mois.